The Vulva
The vulva is the external female genital complex — mons pubis, labia majora and minora, clitoris, vestibule (including urethral meatus, vaginal introitus, Bartholin and Skene gland openings), vestibular bulbs, and perineal body. For the reconstructive pelvic surgeon it is the junction organ between the anterior compartment (bladder, urethra, anterior vagina), the perineal body (posterior vagina, rectum, pelvic-floor attachments), and the external skin envelope — which means nearly every pelvic operation either traverses it, anchors to it, or must protect it. The clinically decisive anatomy is the clitoral neurovascular bundle, the pudendal terminal branches and Alcock's canal, the perineal body and its fibromuscular converging structures, and the fascial continuity with Colles' and Scarpa's fasciae. This article focuses on that anatomy, with physiology and embryology compressed to what a reconstructive surgeon needs to reason about sensory outcomes, sexual function after surgery, and fistula / SCC / LS territory.
See also Vaginal Anatomy for structures proximal to the introitus; Female Urethra for the sphincteric anatomy at the anterior vestibule; and Perineum for the perineal body and superficial/deep pouches.
Gray's Anatomy Fig. 589 — External genital organs of the female.
Components (external → medial)
| Structure | Key features | Operative relevance |
|---|---|---|
| Mons pubis | Fatty pad over pubic symphysis; hair-bearing after puberty | Flap territory for neovagina lining and for genitoplasty |
| Labia majora | Hair-bearing, fat- and sebaceous-gland-rich, homolog of the scrotum | Donor site for Martius labial-fat-pad flap; vulvectomy and reconstruction territory |
| Labia minora | Thin, hairless, sebaceous; highly variable in size (length 20–100 mm, width 7–50 mm)[5]; merge anteriorly as clitoral hood / frenulum and posteriorly at the posterior fourchette | Labiaplasty, vestibulectomy, clitoral-hood reconstruction; territory for vaginoplasty lining flaps |
| Clitoris | Glans + body + paired crura (see below) | The focus of sensory preservation in every genital operation |
| Vestibule | Bounded by Hart's line laterally; contains urethral meatus anteriorly and vaginal introitus posteriorly; openings of Bartholin glands at 5 and 7 o'clock and Skene (paraurethral) glands alongside the urethral meatus | Site of vulvodynia (vestibulodynia), urethral-diverticulum access, Bartholin-gland procedures |
| Vestibular bulbs | Paired erectile structures lateral to the vaginal opening, homolog of the corpus spongiosum[4][6] | Sexual response; dissection margin during vestibulectomy |
| Perineal body | Fibromuscular convergence zone between the introitus and anus (~20–40 mm craniocaudal)[3] | Anchors bulbospongiosus, superficial and deep transverse perinei, external anal sphincter, and posterior vaginal fascia; the reconstructive target of perineorrhaphy and the damaged structure in OASIS lacerations |
The Clitoris — the Dominant Sensory Structure
The clitoris has three continuous components:[2][6][7]
| Component | Dimensions | Tissue type |
|---|---|---|
| Glans | ~5–12 mm long, 3–10 mm wide | No erectile tissue; extraordinarily high nerve density |
| Body (shaft) | ~13–59 mm long, 5–14 mm wide; sits under the mons pubis / clitoral hood | Paired corpora cavernosa with tunica albuginea |
| Crura | 25–68 mm long, paired, attached to the ischiopubic rami | Erectile corpora cavernosa continuous with the body |
Key anatomical facts that drive operative behavior:
- The clitoris is substantially larger than its visible component. Most of its mass is the body and the paired crura, which run along the inferior pubic rami deep to the labia majora and the bulbospongiosus.
- The clitoral neurovascular bundle (dorsal nerve and dorsal artery of the clitoris, paired) runs on the dorsal aspect of the clitoral body within Buck's-fascia-like investing tissue, immediately adjacent to the medial periosteum of the inferior pubic ramus. Jackson et al.'s histologic study measured the dorsal nerve at 2–4 mm at the level of the crura and 1–2 mm at the distal body — not a nerve that tolerates blunt dissection.[7]
- Nerve density gradient — dorsal > ventral along the body; highest in the glans, which is why partial clitorectomy with glans preservation is so much more sensation-preserving than total.[7]
- Nerve density on the labia minora increases distally toward the introitus — a practical detail for labiaplasty incision design.[7]
Clitoral NVB — "the dorsal nerve is periosteal". During any operation approaching the clitoral body or crura (vestibulectomy, urethral-diverticulum repair, radical vulvectomy, gender-affirming vaginoplasty / metoidioplasty, clitoral reconstruction after FGM), the dorsal nerve of the clitoris runs adherent to the periosteum of the inferior pubic ramus along the dorsomedial surface of the crus and body. Stripping the neurovascular bundle off the ramus en bloc with its investing fascia preserves sensation; dissecting on the corporal surface transects fine branches and compromises it.
Innervation
The vulva has sensory, autonomic, and motor innervation, with the clinically decisive supply being the terminal branches of the pudendal nerve (S2–S4):[8][11]
| Branch | Destination |
|---|---|
| Dorsal nerve of the clitoris | Clitoris (glans dominantly) — the dominant sensory supply to the organ |
| Perineal (posterior labial) nerves | Labia majora/minora and vestibule |
| Inferior rectal nerve | Perineum, perianal skin, external anal sphincter |
The pudendal nerve courses through Alcock's (pudendal) canal on the medial surface of the obturator internus along the ischial spine and sacrospinous ligament — the site of pudendal-nerve block, pudendal entrapment syndrome, and the anatomic caution during sacrospinous-ligament fixation (SSLF) and pudendal-canal decompression.
Ilioinguinal (L1) and genitofemoral (L1–L2) branches also supply the mons and anterior labial skin, paralleling their male equivalents.
Autonomic innervation arrives via the inferior hypogastric (pelvic) plexus:
- Parasympathetic (S2–S4, pelvic nerve) → erectile function of the clitoral body/crura and vestibular bulbs; glandular secretion (Bartholin, Skene).
- Sympathetic (T10–L2, hypogastric nerve) → vasoconstriction and default tone.
Motor innervation — perineal branches of the pudendal nerve drive the bulbospongiosus, ischiocavernosus, and superficial and deep transverse perinei.
Neuroproliferative vestibulodynia (the "red-ring" tender vestibule) is characterised by increased CGRP-positive sensory nerve density and altered VIP/TH autonomic fibers within the vestibule itself — the neuroanatomic basis for vestibulectomy as definitive therapy in selected patients.[9][10]
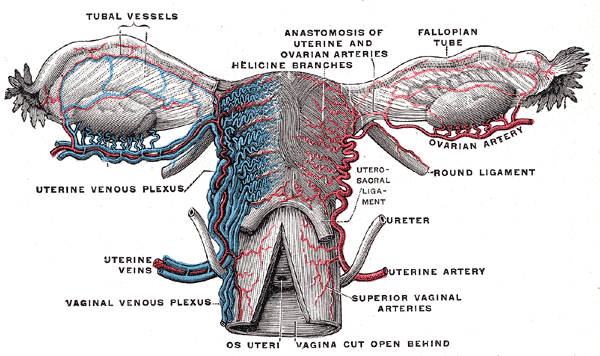
Vascular Supply
- Internal pudendal artery (internal iliac) — via perineal branches; gives deep (cavernosal) and dorsal arteries of the clitoris, posterior labial arteries, and perineal branches. The dominant supply.
- External pudendal arteries (from the femoral) — supply mons and anterior labial skin; the axial vessels for Martius labial flaps.
The Martius labial fat-pad flap exploits the fact that the labium majus receives a reliable, bidirectional blood supply (external pudendal superiorly, internal pudendal inferiorly) — the flap can be based on either pedicle depending on the defect (anterior fistula, mid-anterior-vaginal defect, urethral-wall reinforcement, etc.).
Venous drainage parallels the arteries to the internal and external pudendal veins.
Lymphatic drainage:
- Most of the vulva → superficial inguinal nodes, then deep inguinal and external iliac.
- Clitoris and anterior labia → can drain bilaterally; unilateral vulvar SCC is approached with bilateral inguinofemoral lymphadenectomy when near the midline.
- Deep inguinal (Cloquet's) node is the proximal sentinel for more advanced disease.
Fascial Continuity — Why Hematomas, Infection, and Fournier's Spread Predictably
The dartos fascia of the labia majora is continuous with Colles' fascia (perineal superficial fascia) posteriorly and with Scarpa's fascia of the anterior abdominal wall through the inguinal region. Infection or hematoma in this superficial perineal plane tracks cephalad into the anterior abdominal wall, laterally onto the thigh, and posteriorly along the perineum — but does not cross the urogenital diaphragm into the deep pelvis. This is the anatomic basis of:
- Vulvar hematoma (obstetric, post-traumatic) extension onto the abdominal wall
- Fournier's gangrene of the vulva spreading along dartos / Colles' / Scarpa's in the same way it does in men
- Extravasation of urine after urethral injury confined to this compartment
The testis-analog of the scrotum is the labium majus; the fascial compartmentalisation is identical.
Glands of the Vestibule
| Gland | Location | Clinical correlate |
|---|---|---|
| Bartholin (greater vestibular) | Paired; openings at 5 and 7 o'clock of the vaginal introitus | Bartholin abscess / cyst → marsupialization or Word catheter; recurrent disease → excision (with attention to the nearby internal pudendal vessels); Bartholin gland carcinoma — rare, retromolar mass, radical local excision + inguinal LND |
| Skene (lesser vestibular / paraurethral) | Alongside urethral meatus | Skene gland cyst / abscess; origin of most adult urethral diverticula and of Skene gland carcinoma |
Physiological Functions (kept brief)
- Sensation and sexual response. Parasympathetic activation → vasodilation and engorgement of clitoral body, crura, and vestibular bulbs; labia minora engorge and redden. The glans clitoris is the highest-density sensory surface, and its innervation must be preserved to protect arousal and orgasm.
- Glandular secretion. Bartholin glands contribute a minor fraction of lubrication under parasympathetic drive; Skene glands produce antimicrobial peritrigonal secretion.
- Protection and structural closure. Labia majora close the urogenital cleft at rest; the perineal body anchors the superficial perineal musculature and is a key load-bearing structure of the pelvic floor.
Embryology (compressed)
The external genitalia arise from four paired structures common to all patients: genital tubercle (clitoris or glans penis), urogenital folds (labia minora or ventral penile shaft), labioscrotal swellings (labia majora or scrotum), and urogenital sinus (vestibule and urethra vs prostatic + membranous urethra).[4] The resulting homologies are clinically essential for:
- Disorders of sex development (DSD) and the vocabulary of feminising or masculinising genitoplasty.
- Gender-affirming genital surgery, where labia majora / scrotum, clitoris / glans, and vestibule / urethra each become each other's source tissues in reconstruction.
- Reconstruction after female genital mutilation (FGM) — clitoral reconstruction exploits the preserved subcutaneous clitoral body / crura deep to the scarred glans.
Clinical Correlations for the Reconstructive Surgeon
- Vestibulodynia and vestibulectomy. Provoked vulvodynia localized to the vestibule — particularly the posterior vestibule — responds to complete vestibulectomy with vaginal advancement flap in selected patients. Anatomic basis: CGRP-positive sensory nerve density is pathologically elevated in the affected vestibular mucosa; excising it and bringing down vaginal mucosa restores normal sensory map.[9][10]
- Bartholin pathology. Acute abscess → Word catheter or marsupialization; recurrent cysts → marsupialization, CO₂ laser, or excision. Postmenopausal new Bartholin-area mass — rule out carcinoma by biopsy before drainage.
- Urethral-diverticulum access. Most diverticula originate from obstructed Skene glands, present as a tender midline anterior-vaginal mass, and are approached through a flap-based anterior vaginal wall dissection that mobilizes the urethra, completely excises the sac, closes the urethra in two layers over a catheter, and interposes a Martius labial fat-pad flap when tissue quality or fistula risk warrants.
- Martius labial fat-pad flap. The workhorse interposition flap for:
- Vesicovaginal and urethrovaginal fistula repair
- Urethral diverticulectomy reinforcement
- Complex perineal wound coverage Harvested through a vertical labia-majora incision based either on the posterior labial branch of the internal pudendal (inferiorly pedicled) or on the external pudendal (superiorly pedicled); choice depends on the destination defect.
- Clitoral reconstruction. After FGM/C (reattachment and uncovering of the preserved body/crura), after oncologic resection, or as part of gender-affirming surgery (metoidioplasty / vaginoplasty). Preservation of the dorsal nerve of the clitoris is the limiting technical step in all of these.
- Vulvar SCC. ~90% of vulvar malignancies; two biologic pathways (HPV-associated and non-HPV/LS-associated). Operations range from wide local excision (superficial lesions) to radical vulvectomy with inguinofemoral lymphadenectomy; sentinel node biopsy has largely replaced complete groin dissection for small, unifocal, <4 cm lesions with clinically negative nodes.
- Vulvar lichen sclerosus (LS). Chronic inflammatory dermatosis driving introital narrowing, clitoral hood fusion, and distal urethral stenosis; long-term risk of HPV-negative vulvar SCC. Medical management is high-potency topical corticosteroids; surgical reconstruction (clitoral hood release, introital widening with Y-V flap or graft) addresses the scarring consequences.
- Obstetric anal sphincter injury (OASIS) and perineorrhaphy. 3rd-degree (sphincter involvement) and 4th-degree (rectal mucosa) tears destroy the converging structures of the perineal body. Repair rebuilds external anal sphincter, internal anal sphincter (when disrupted), and the perineal-body convergence of bulbospongiosus and transverse perinei.
- Female genital reconstruction after cancer therapy. Post-radiation vulvar stenosis and fistula are common sequelae of pelvic-cancer treatment; reconstruction uses Martius, Singapore (pudendal-thigh) fasciocutaneous, gracilis, or VRAM flaps depending on defect size and irradiated bed.
- Gender-affirming vulvoplasty / vaginoplasty. Creates a clitoris from the glans penis (dorsal-nerve-preserved neurovascular pedicle), labia minora from the dorsal penile skin, labia majora from scrotal skin, and vestibule / neovaginal canal from penile shaft skin / scrotal graft / intestinal segment — a direct reversal of the embryologic homologies.
- Vulvar hematoma and Fournier's. Both track along the dartos / Colles' / Scarpa' continuum; know the boundary (urogenital diaphragm) and the anatomic routes of spread for diagnostic and debridement planning.
- Pudendal nerve block and entrapment. Landmarks are the ischial spine and sacrospinous ligament for transvaginal / transperineal block; entrapment in Alcock's canal presents as neuropathic vulvar / clitoral / perineal pain and is treated with decompression in refractory cases.
References
1. Golden E, Cooke S, Butler E, Gregg L, Gomez E. "Under the Hood: Vulvar Anatomy and Pathology With a Focus on MRI." Abdom Radiol (NY). 2026;51(4):2106–2124. doi:10.1007/s00261-025-05179-1
2. Yeung J, Pauls RN. "Anatomy of the Vulva and the Female Sexual Response." Obstet Gynecol Clin North Am. 2016;43(1):27–44. doi:10.1016/j.ogc.2015.10.011
3. Committee on Practice Bulletins-Obstetrics. "ACOG Practice Bulletin No. 198: Prevention and Management of Obstetric Lacerations at Vaginal Delivery." Obstet Gynecol. 2018;132(3):e87–e102. doi:10.1097/AOG.0000000000002841
4. Puppo V. "Embryology and Anatomy of the Vulva: The Female Orgasm and Women's Sexual Health." Eur J Obstet Gynecol Reprod Biol. 2011;154(1):3–8. doi:10.1016/j.ejogrb.2010.08.009
5. Kreklau A, Vâz I, Oehme F, et al. "Measurements of a 'Normal Vulva' in Women Aged 15–84: A Cross-Sectional Prospective Single-Centre Study." BJOG. 2018;125(13):1656–1661. doi:10.1111/1471-0528.15387
6. Tappy EE, Corton MM. "Anatomy of Sex: A Review of Critical Structures Within the Vulva and Vagina." J Minim Invasive Gynecol. 2026;33(1):3–9. doi:10.1016/j.jmig.2025.08.022
7. Jackson LA, Hare AM, Carrick KS, et al. "Anatomy, Histology, and Nerve Density of Clitoris and Associated Structures: Clinical Applications to Vulvar Surgery." Am J Obstet Gynecol. 2019;221(5):519.e1–519.e9. doi:10.1016/j.ajog.2019.06.048
8. Choi BJ, Chung MS, Chung BS. "Pudendal Nerve Identified on Sectioned Images of Female Cadaveric Pelvis." Urology. 2020;142:76–80. doi:10.1016/j.urology.2020.05.007
9. Tomalty D, Giovannetti O, Magliocchetti S, et al. "Characterizing the Innervation of the Vulvar Vestibule and the Immunohistochemical Features of Neuroproliferative Vestibulodynia." J Sex Med. 2023;20(6):716–731. doi:10.1093/jsxmed/qdad040
10. Velikonja L, Giovannetti O, Adams MA, Tomalty D. "Innervation of the Human Vulvar Vestibule: A Comprehensive Review." Clin Anat. 2023;36(1):18–27. doi:10.1002/ca.23966
11. Yucel S, De Souza A, Baskin LS. "Neuroanatomy of the Human Female Lower Urogenital Tract." J Urol. 2004;172(1):191–195. doi:10.1097/01.ju.0000128704.51870.87